The UK is one of the better-prepared countries, at the moment, to deal with Covid19. As per data published by the official website, 89.7% of the UK population, aged 12yr and above, have already taken at least one dose of vaccine, whereas 53% have taken three (data on 23/12).
It would be interesting to see how the country is doing so far against the virus. The following plot gives you various health-related parameters of Covid 19 infection. Critical parameters such as hospitalisations and deaths have been rescaled – both x and y axes – to coincide with the reported cases before the vaccine.
These are not perfect but are analyses capable of providing semi-qualitative insights. The peak rates in later 2020 – early 2021 suggest a case fatality ratio of about two (1 in 50) and a hospital admission case of 1 in 15. This was the situation before the vaccines became available. The ratios have come down significantly since then.
I was not originally planning to write this piece here. It just happened as an immune response to a fast-spreading youtube virus.
What is the debate?
The argument of the youtube virus was: “vaccines protect from illness. It is well-known that the current vaccines are not stopping the disease from spreading. The current vaccines only manage the condition from becoming worse. Therefore, they are not vaccines, and the system is cheating people”. He also uses a fallacy called theappeal to authority and invokes high-profile personalities from the Indian Council of Medical Research to support his view (I didn’t think a fact-check was necessary; evidence should lead and not personalities).
The vaccinated are getting infected!
I have made two posts already to show using data that the current vaccines are just delivering as they promised. Also proved mathematically, the reason for the large number of breakthrough infections for Covid, while there are near-zero levels for those vaccinated against traditional illnesses. Some of the old vaccines appear so good because their prevalence is negligible these days. Once you view the present-day covid vaccines in that light (of super high prevalence in society), you appreciate the work they are doing.
Infection vs Disease
Infection happens when pathogens (bacteria, viruses, others) enter the body and multiply. So what can prevent an infection? A barrier around your nose and mouth or by staying at home! On the other hand, disease occurs when the infection begins damaging cells. The signs of symptoms appear, and the body’s immune system acts. It is worth noting that many of the symptoms result from the activities of the immune system; fever is a well-known one.
Prevention vs Mitigation
These are two terms typically used in risk management. Their definitions are below (taken from OALD).
Prevention: the act of stopping something bad from happening. Mitigation: a reduction in how unpleasant, serious, etc. something is.
It is easy for humans to jump into the binary of prevention vs mitigation, or vaccine vs medicine. But life is more than such binaries and is full of things in between. Say the risk of getting a stroke. Doing exercises, eating balanced food, and leading a healthy lifestyle are considered prevention strategies. Suppose you have high blood pressure and you take medicines to control it. You may call it mitigation to the condition called high blood pressure. Or it can also be prevention for the real issue, the chance of getting a stroke or a heart attack or a kidney failure. In other words, prevention vs mitigation becomes a philosophical debate.
A boost to immunity?
The most useless definition of how vaccines work is boosting immunity. As a scientist, you want better. What about this: vaccines trigger immunise response in the body? It sounds better, but what is that?
When pathogens enter the body, they attach to the cell and use their resources to multiply. While all the cohabitant microbes do these (the human body has more microbes than the number of cells), only a few guys are called pathogens for a reason. They spit out antigens that can cause harm to the cell. The body uses a few techniques to mitigate this. Yes, ‘mitigate’ is my word of choice, from the viewpoint of the antigen, but you may use ‘prevent’ from the cell’s point of view. The body may respond with fever (heat inactivates many viruses), a chemical called interferon (which blocks viruses from reproducing), or deploy antibodies and other cells to target the invader.
How do Covid vaccines work?
Most of the Covid vaccines are targetting the production of antibodies against spike proteins. The antibodies, produced by the body, connect to the anchor points of the virus (the spikes), nullify the attachment of the latter, and eventually its proliferation.
One thing is clear: you need to somehow get antibodies to where it is required. Many new-generation covid vaccines work by transferring the genetic information – that produces the protein-spike – to our cells, either through messenger RNAs or by inserting it inside other viruses. Once the body gets the code, it starts making spike proteins, and antibodies follow.
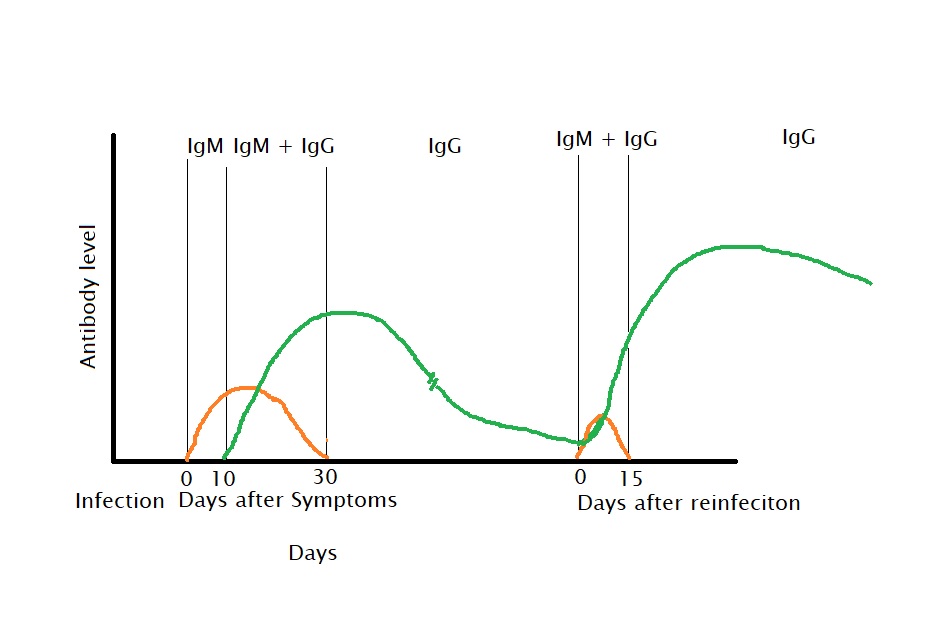
Infection and Reinfection Curves
A simple schematic of antibody production. The numbers are indicative and may vary from person to person or from disease to disease.
Several publications are available that quantify antibodies produced from various covid vaccines. To give a personal touch, the following are data from my blood tests, taken at three different intervals after my vaccine jabs.
Test done in July 2021Test Done in August 2021Test done in November 2021
Laws of mass action – What makes the debate possible?
The reaction rate between A and B forming a product is proportional to their concentrations and rate constant. The higher the concentrations or the rate constant, the faster is the reaction. Any standard chemistry textbooks will give you details. Four reactions are important to consider – the first two are against us, and the last two are with us. 1) virus + resources -> 2 virus, 2) virus + cell -> destruction. 3) blood plasma -> antibodies 4) virus + antibody -> safe product. We want items 3 and 4 to happen faster than 1 and 2.
Suppose an individual gets exposed to a high viral load. It makes the virus concentration of reactions 1 & 2 high and forces the reactions to go faster. The reaction that matters the most, reaction-4, will take some time as the amount of antibody, in the beginning, is zero. If the first reactions manage to destroy more cells, you are in big trouble. This is the trouble with Covid19; it multiplies faster and has a high sticking tendency due to its spikes.
What is the end goal of the debate?
The virus is ubiquitous now that you can see all possible ways it demonstrates in public – from people who get up without any symptoms to people dying even after getting multiple doses of vaccines. We are talking about hundreds of millions of bodies carrying out these reactions in real time. Whenever that happened in the past, they took millions of life along with them.
You will never know the real goal of the debate, but I can tell you the result. It is confusion, mistrust in the system and ultimately vaccine hesitancy. These are proving, once again, that it is easy to confuse people, by using well-known facts, but by taking them out of context and making a louder noise.
Is it prevention or mitigation? The question is not valid, and it is not either-or. Prevention and mitigation are just viewpoints that we might get based on your body’s performance. These vaccines are like any other vaccine; their job is to provide scenarios of the first infection, and are our best weapon to fight the disease, so get it. There are hundreds of data, not opinions, available in public space that support this. The only difference this time? The lab work is happening in front of you, with spotlights on!
Further Read
Safety and immunogenicity of the ChAdOx1 nCoV-19 vaccine: The Lancet
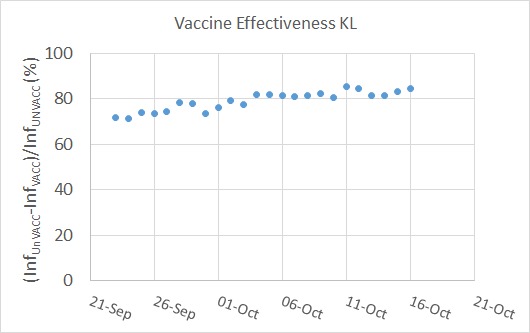
I have shown you my estimates on vaccine effectiveness in Kerala in an earlier post. The plot is reproduced below.
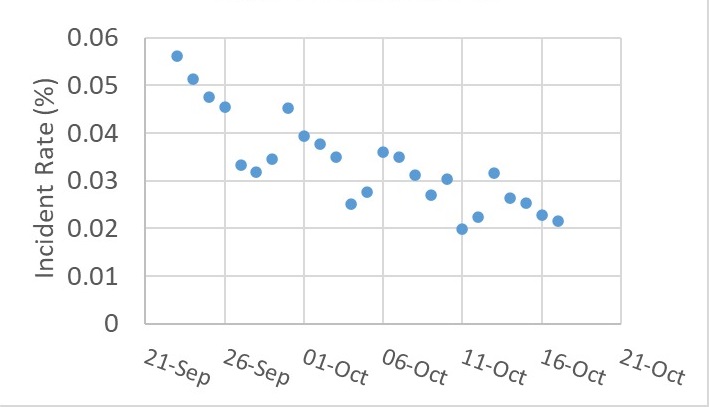
You may have noticed that the effectiveness was steadily going upwards. Intrigued, it has prompted me to check what was going on with the other variables during the same period. One of them was the overall incident rate (shown below).
Puzzled by those periodic minima in the plot? It is an artefact in the data caused by the lower-than-usual number of tests on Sundays!
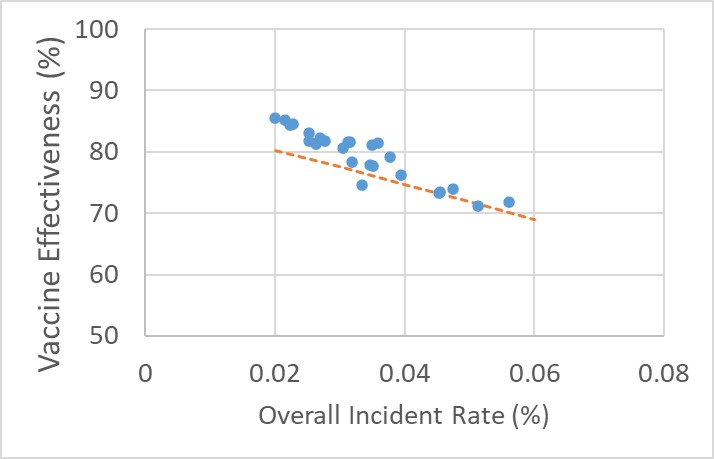
Yes, you guessed it right: the next step is to plot the incident rate with vaccine effectiveness. As expected, it is a straight line!
Correlation or Causation
It was still not easy to know what was happening. The whole observation can be a confounded outcome of something else. We have seen how chance plays its role in containing the disease outbreak (the post of swiss cheese!).
The next logical step is to perform the calculations and check if the trends are making sense. The calculations are:
Let P be the prevalence of the disease (incidence rate multiplied by some number to cover the who can still infect others at a given time). V represents the holes in the vaccination barrier, U is the holes in the unvaccinated (probability = 1), M is the holes in the mask usage, and n is the number of exposures that a person encounters. Here, I’ve stopped at mask as the only external factor, but you can add more barriers such as safe distance.
The chance of getting infected in n encounters with the virus = (1 – chance of being lucky in n encounters) The chance of getting lucky in n encounters is = nCn x (chance of being lucky once)n x (chance of being unlucky once)0 = (chance of being lucky once)n.
The probability of being lucky once = (1 – chance of getting infected in a single encounter). The chance of getting infected is the joint probability of breaking through multiple barriers. So luck = (1 – P x M x V) for a vaccinated person and (1 – P x M) for an unvaccinated person. Note that V is related to 1 – prior assumed efficacy of the vaccine.
Finally, the effectiveness of vaccine = { [1 – (1 – P M )n] – [1 – (1 – P M V)n] } / {1 – (1 – P M)n}
You can already see from the expression that the vaccine effectiveness is a function of P, the prevalence. Repeat the calculations for a few incidence rates, and the results are plotted along with the actual data. The dotted line represents the estimation.
Key Takeaways
An apple to apple comparison between vaccines requires, among other things, the prevalence of the disease during the period of the efficacy trials. Part of the reason why many of the Covid 19 vaccines are showing modest efficacy levels lies in the extraordinary high incident rate of the illness prevailing through the last year and a half. A high prevalence of disease in society means a person, even though vaccinated, would encounter the virus several times, increasing the probability to get infected. Every such event is an additional test to the efficacy.
The COVID-19 pandemic presented us with a live demonstration of science at work, much to the surprise of many who are not regular followers of its history. It gave a ringside view of the current state of the art, yet it created confusion among people whenever they missed consistency in the messaging, theories, or guidelines. The guidance on protective barriers—using masks, safe distancing, and hand washing—was one of them.
Swiss Cheese Model of Safety
The Swiss cheese model provides a picture of how the layered approach of risk management works against hazards. Let us use the model to check the underlying math behind general health advice on COVID-19 protection. I describe it through a simplified probability model.
The probability of someone getting infected by Covid 19 is a joint probability of several independent events. They are the probabilities:
an infected person who can transmit the virus in the vicinity (I)
to get inside a certain distance (D)
to pass through a mask (M)
to pass through the protection due to vaccination (V)
to get the infection after washing hands (H)
to infect the person once the virus is inside the body (S)
Infected person in the vicinity (I): is equal to the prevalence of the disease (assuming homogeneous mixing of people). Let’s make a simple estimate. These days, the UK reports about 50,000 cases per day in a population of 62 million. It is equivalent to an incident rate of 0.000806. Assume that an infected person can transmit the virus for ten days, and half of them manage to isolate themselves without passing the virus to others. The prevalence (proportion of people who can transmit the disease at a given moment) is 5 x 0.000806 = 0.0004032. Multiply by a factor of 2 to include the asymptomatic and the symptomatic but untested folks too into the mix. Prevalence becomes = 0.0008064 (8 in 1000).
To get inside a certain distance (D): If the person managed to stay outside the 2 m radius from an infected person, there could be zero probability of getting infected, but it is not practically possible to follow every time. Therefore, we assume she managed to stay away 50% of the time, which means a probability of 0.5 to get infected.
To pass through a mask (M): General purpose masks never offer 100% protection against viruses. So, assume 0.5 or 50% protection.
To pass through the protection from vaccination (V): The published data suggest that vaccination could prevent up to 80% of symptomatic infections. That means the chance of getting infected is 0.2 for the vaccinated.
The last two items – hand washing (H) and susceptibility to getting infected (S) – are assumed to play no role in protecting COVID-19. Infection via touching surfaces plays a minor role in transmission, and the latest variants (e.g. Delta) are so virulent that almost all get it once it is inside the body.
Assume a person makes one visit outside in a day. The probability of getting the infection is = I x D x M x V x H x S = 0.008 x 0.5 x 0.5 x 0.2 x 1 x 1 = 0.0004 or the chance of not getting is 0.9996.
The person makes one visit for 30 days (or two visits for 15 days!). Her probability of getting infected on one of those days is = 1 – the probability she survived for 30 days. To estimate the survival probability, you need to use the binomial theorem. Which is 30C30 x 0.999630 x 0.0040 = 0.988. The chance of a fully protected person getting infected in a month outdoors is 1 – 0.988 or 12 in 1000!
Scenario 2: Fully Protected Person Indoor
The distance rule doesn’t work anymore, as the suspected droplets (or aerosols or whatever) are available everywhere. The probability of getting the infection is = I x D x M x V = 0.008 x 1 x 0.5 x 0.2 = 0.0008. This means the chance of not getting is 0.9992. 30-day chance is 1 – 0.976 = 0.024 or 24 in thousand.
Scenario3: Indoor Unprotected but Vaccinated
I x I x D x M x V = 0.008 x 1 x 1 x 0.2 = 0.0016. The chance of getting infected in a month = 1 – 0.95 or 5 in hundred.
Scenario4: Indoor Unprotected
I x D x M x V = 0.008 x 1 x 1 x 1 = 0.008. The chance of getting infected in a month = 1 – 0.78 or about 2 in 10 chance.
A bunch of simplifications were made in these calculations. One of them is the complete independence of items, which may not always hold. Some of these can be associated – a person who cares to make a safe distance may be more likely to wear a mask and get vaccinated. Inverse associations are also possible – a vaccinated person may start getting into crowds more often and stop following other safety practices.
Second is the simplification of one outing and one encounter with an ill person. In reality, you may come across more than one infected. In the case of indoor, the suspended droplets containing the virus act as encounters with multiple individuals.
The case of health workers is different as the chances of encountering an infected person in a clinic or a medical facility differ from that in the general public. If one in ten people who come to a COVID clinic is infected, the chances of the health worker getting infected in a month are 95% if she wears an ordinary mask and comes across 100 patients daily. If she uses a better face cover that offers ten times more protection, the chance becomes about 25% in a month, or one in 4 gets infected even after getting vaccinated.
Bottomline
Despite all these barriers, people will still get infected. Small portions of large numbers are still sizeable numbers but do not get distracted by them. Use every single protection that is available to you. Those include vaccination, mask use, maintaining distance, and reducing non-essential outdoor trips. They all help to reduce the overall rate of infection.
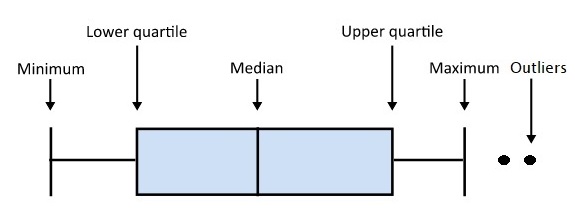
The boxplot is my favourite plot. The plot can summarise and maintain the statistical perspective by showing the data distribution. So, what is a boxplot? The following picture explains it.
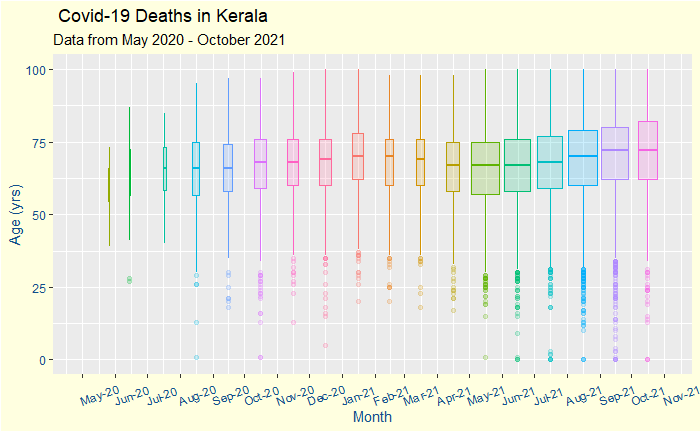
Now, let’s apply the plot to COVID-19 deaths. The data summarises the distribution of COVID deaths from its beginning. Data comes from the Covid dashboard of the Government of Kerala.
First, it is a time series organised monthly. The box’s width represents the total number of deaths in that month. The ‘boxes’ take you through the time of the first wave and the second one caused by the Delta (B.1.617.2) variant.
Broad Observations
The number of deaths shot up from May 2021, the start of the fast-spreading second wave of infection.
The median age of the deceased did not show any reduction after May 2021 (after the arrival of the delta), dismissing speculations on the deadliness of the new strain.
The median age of death marginally dropped starting in March, which coincided with the vaccination program for the elderly. The number systematically increased after June, coinciding with the younger population taking the vaccination. Note that these are correlations and do not necessarily mean causations!
Deaths for people below the age of 35 years do happen but are rare outliers in the statistics.
The incidence of death may be beginning to ease out towards the end.
If you like the boxplot, here is your bonus plot
The new plot includes the actual data points. More men have died from the disease, and for whatever reason, their median age at death is also a couple of years lower than women.
A news item broke out in October 2021 on the vaccination program in Kerala (India). The journalist on screen was ‘shocked’ at the daily report of 6525 vaccinated and 2802 unvaccinated in the group of 9327 infected adults. Infection numbers among the vaccinated people outnumbered the unvaccinated. And it raised serious doubts over how the state managed the vaccination program.
Let’s try and understand what these numbers mean.
Infection Risks
The number of adults infected in the vaccinated: 6525 The total vaccinated adults in Kerala (at least one dose): 25.01 million Infection risk for the vaccinated: (6525 / 25,010,000)x100 = 0.026%
The number of infected adults in the unvaccinated: 2802 The number of unvaccinated adults on that date: 1.68 million Infection risk for the unvaccinated: (2802 / 1,680,000)x100 = 0.167%
Vaccine effectiveness: (difference in infection risk between unvaccinated and the vaccinated) / infection risk of the unvaccinated = (0.167-0.026)/0.167 = 84%, not bad, heh?
We can repeat the exercise for a month to get a statistical perspective. Here is what I get
I did not use the word efficacy to describe my results, though I used the math behind that calculation. Estimating vaccine efficacies requires a more careful analysis of the infection data, something I leave to the experts in the field. What I did here is a preliminary assessment to make sense of the journalist. And the analysis suggested that the vaccine did what it promised.
Remember our theme?: life is about chances, rationality, and decision-making.
“In the long run, we are all dead” John Maynard Keynes
Rewind your memories to August of last year (2020). The Oxford group have just published a landmark report, ChAdOx1 nCoV-19 vaccine against SARS-CoV-2 (20th July in Lancet). For the planet that was reeling under Covid 19, it was a rare piece of good news.
Vaccines and Side Effects
Fast-forward a year, and the world has a few more candidates, and everyone expects vaccination to start in full steam. But the excitement has partly given way to confusion and scepticism. The news of rare blood clots dominated the news, governments gave conflicting guidance, and the public was puzzled. And the anti-vaxxers got more ammunition for their kitty.
Perceptions of Risk in Life
Life is not risk-free. Let us start with the birth of a person: the chance of a child dying at birth in the US is 6 in 1000, 28 in India, 2 in Japan, etc. Once you survive that risky event, you get a 5 in a million chance of dying from murder, 100 in a million in road accidents, and 170 in a million pregnancy-related (all in the US). That, too, without considering the leading causes of death, namely heart disease and cancer. Does that prevent anyone from giving birth or travelling by road?
The Life of Trade-Offs
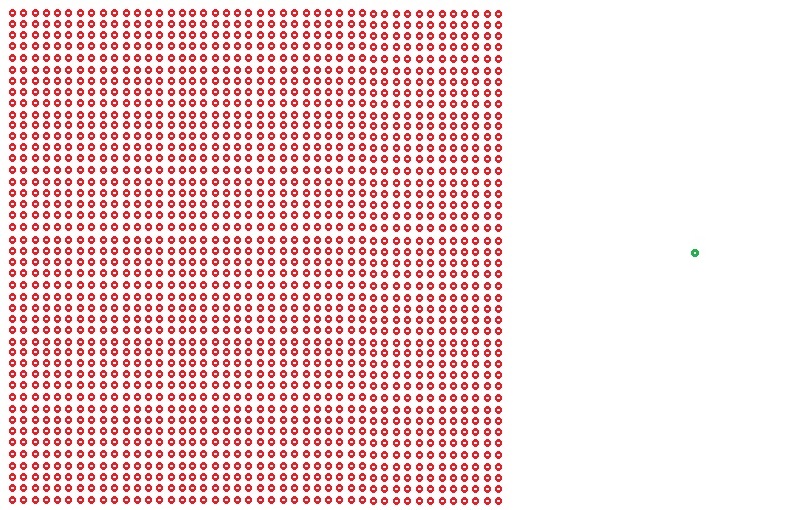
Consider this: 740,000 of the total 330 million population are dead in the US (as of today, 28/10/2021) due to COVID-19. It is not clear what proportion of the total population was infected. In other words, 0.74 in 330 (0.2 % or 2 in thousand) is a reasonable estimate of the risk of dying due to COVID-19. A similar calculation for India is 3 million deaths (from the median estimate for excess deaths in 2020-21, from various scientific assessments such as the one by Deshmukh et al., MedRxiv) of the total 1400 mln population. The ratio comes out to be 0.21%. A similar estimate for the UK is 140,000 (official count as of today) out of a population of 67 million, also 0.2%. Brazil is 0.28%, and the list goes on. Note that this represents the average risk of dying from COVID-19 (averaged over age, incident rate, comorbidities, suggesting that the case fatality ratio can only be higher).
[in fact, 0.2% seems so powerful that it is a good measure of identifying “cheaters” in this pandemic!]
Now, what is the chance of dying due to vaccination? Based on various studies, it is about 1 in a million, slightly more than being struck by lightning in a given year in the US (1 in 1,222,000). So the comparison is between 2 in a thousand and 1 in a million. Or, it is a comparison between 2000 and 1. That is the trade-off you must make. What will you do?
Death due to Infection (red) vs Death by Vaccine (green)
And that is where we humans sometimes lose perspective.
PS: The author and his family are happy recipients of the ChAdOx1 nCoV-19 vaccine.